

Autumn Study Day 2025
John Prendergast, CSC Chair, opened the Autumn Study Day with a warm welcome to North Wales – and welcome to Hollywood! with today being one that celebrates science, collaboration, and community.
John expressed his pleasure at bringing the CSC back to Wales. Our last visit was in 2018 for the Annual Scientific Meeting in Cardiff.
Spotlight on Wrexham
North Wales is a region of contrasts: rugged mountains, industrial heritage, coastal beauty, and rural charm. Wrexham, often called the capital of North Wales, boasts a rich history in coal mining, steel, brewing, and now aerospace manufacturing.
The area has seen its share of hardship – notably the Gresford mining disaster of 1934, which claimed 200 lives. Yet today, Wrexham is enjoying a renaissance, thanks to Hollywood stars Ryan Reynolds and Rob McElhenney, whose investment in Wrexham AFC has captured hearts across Britain. Football fans from Liverpool and Manchester now flock here to support a true community club.
Famous Faces from North Wales
Wrexham and its surroundings have produced some remarkable talent:
- Tim Vincent – former Blue Peter presenter
- Hugh Griffith – Oscar-winning actor (Ben Hur, The Wild Geese)
- Andy White – drummer on The Beatles’ “Love Me Do”
- Mickey Thomas – scorer of that unforgettable FA Cup goal against Arsenal in 1992
- Jade Jones – double Olympic gold medallist in Taekwondo
This region truly punches above its weight!
A Record-Breaking Event
The days turnout was phenomenal! It had been planned for 80–90 attendees based on previous years, but this event sold out in the first week of September – a testament to the members and non-members enthusiasm for CSC. Thank you for your support!
Turning the Tide: From Ugly Duckling to Beautiful Swan
A Positive Outcome from a JAG Standard Audit
The latest update from across North Wales showcases a remarkable transformation within endoscope decontamination services—an inspiring example of collaboration, perseverance, and commitment to patient safety.

John Prendergast opened the session with an overview of the rigorous audit process undertaken by Shared Services across all main health board endoscopy units. Working alongside Bowel Screening Wales and the All Wales National Endoscopy Programme, these audits follow the standard IHEEM/JAG tool and are instrumental in driving service improvements.
Back in 2018, the endoscopy department at Betsi Cadwaladr University Health Board (BCUHB) was flagged as a red risk in the All Wales Endoscope Decontamination Survey. The concerns were significant: limited space, congestion, ageing and obsolete machinery, deteriorating infrastructure, and facilities far below required standards. Follow‑up JAG audits in 2021 and 2022 continued to highlight these issues, with photos revealing makeshift fixes such as a ventilated peracetic acid cabinet modified by cutting vents into its side, open drains contributing to poor air quality, and manual cleaning areas with inadequate setup.
Despite recurring audit findings, progress initially remained slow. But in 2023, the Health Board acknowledged the pressing need to address the risks—particularly to staff safety—and began working with key partners including NHS Wales Shared Services, Bowel Screening Wales, JAG, and government stakeholders. A new space was identified, and planning began.
A Region-Wide Perspective
Ursula Moby introduced Sandra Jones (Operational Decontamination Lead) and Sian (Operational Lead Sister), who shared insights from this major improvement project across the vast geography of North Wales—spanning six counties from Anglesey to Wrexham.
BCUHB operates three integrated healthcare sectors—West, Central, and East—each with its own acute hospital sites. Ysbyty Gwynedd in the West, Ysbyty Clwyd in the Central region, and Wrexham Maelor in the East all run their own sterile services and endoscopy departments. These wide‑ranging sites face differing challenges but share a need for safe, compliant decontamination practices.

Identifying the Challenges
Sian outlined the long-standing issues encountered in several facilities:
- Non‑compliant sinks and washer disinfectors
- Poor dirty/clean separation
- Exposed drains and ventilation problems
- External chemical stores
- Incomplete audit trails and recordkeeping
- Layouts misaligned with JAG/IHEEM requirements
Beyond the infrastructure, Sian highlighted a cultural challenge: decontamination often perceived as a “Cinderella service,” with staff receiving little recognition despite the complexity and critical importance of their work.
The Case for Change
Sandra emphasised key drivers behind the transformation project:
- Risks to patient safety and service quality
- Repeated audit failures
- Inefficient reprocessing and delays
- Need for compliance-driven investment
- Long‑term cost benefits outweighing ongoing risks
Wrexham Maelor Hospital, opened in 1986, has seen numerous add-on buildings and temporary solutions over the years—including the installation of modular theatres in 2015. A previously allocated endoscopy reprocessing area had remained unused due to logistical and cost concerns, eventually being taken over as a storeroom.
Designing a Modern, Compliant Facility
A multidisciplinary project team was formed, bringing together estates, capital development, the endoscope washer supplier, decontamination staff, the AE(D) team, Health & Safety, and Welsh Government representatives.
Key goals included compliance with JAG and IHEEM standards, a clear set of project milestones, and phased delivery. Staff feedback played an important role—such as ensuring natural light through the inclusion of a window.
The new modular unit now features:
- A compliant dirty‑to‑clean workflow
- Four new washer disinfectors (plus capacity for a fifth)
- Modern sinks, drying cabinets, and appropriate storage
- Enhanced ventilation
- Step‑down water filtration
- Infection‑control‑driven design, including stainless steel surfaces, spill kits, and dedicated handwashing stations
Staff received training on new equipment, standard operating procedures were updated, and a phased transition ensured minimal disruption and maximum staff engagement. Real‑time troubleshooting by Sandra, Sian, estates, and facilities teams helped smooth the early days of operation.
Lessons Learned
The team reflected on important insights:
- Early stakeholder engagement is crucial—particularly around drainage and water supply to washer disinfectors.
- IT and Data teams should be involved sooner.
- Purchasing electronic track and trace alongside washer disinfectors would have prevented reliance on paper systems.
- Early staff involvement builds ownership, reduces resistance, and supports a smoother service transition.
Looking Ahead
Future plans include:
- A six‑monthly audit programme to maintain compliance with IHEEM and BCUHB standards
- Ongoing staff training and competency checks using the BCUHB training matrix
A Successful Transformation
The journey from non‑conformance to a fully compliant endoscope decontamination service has been significant. The project has delivered measurable quality and safety improvements and stands as a model of effective cross‑departmental collaboration.
Or, as Henry Ford famously said:

“If you always do what you’ve always done, you’ll always get what you always got.”
This project shows what is possible when organisations commit to doing things differently.
From Single Colonies to Biofilm Cities

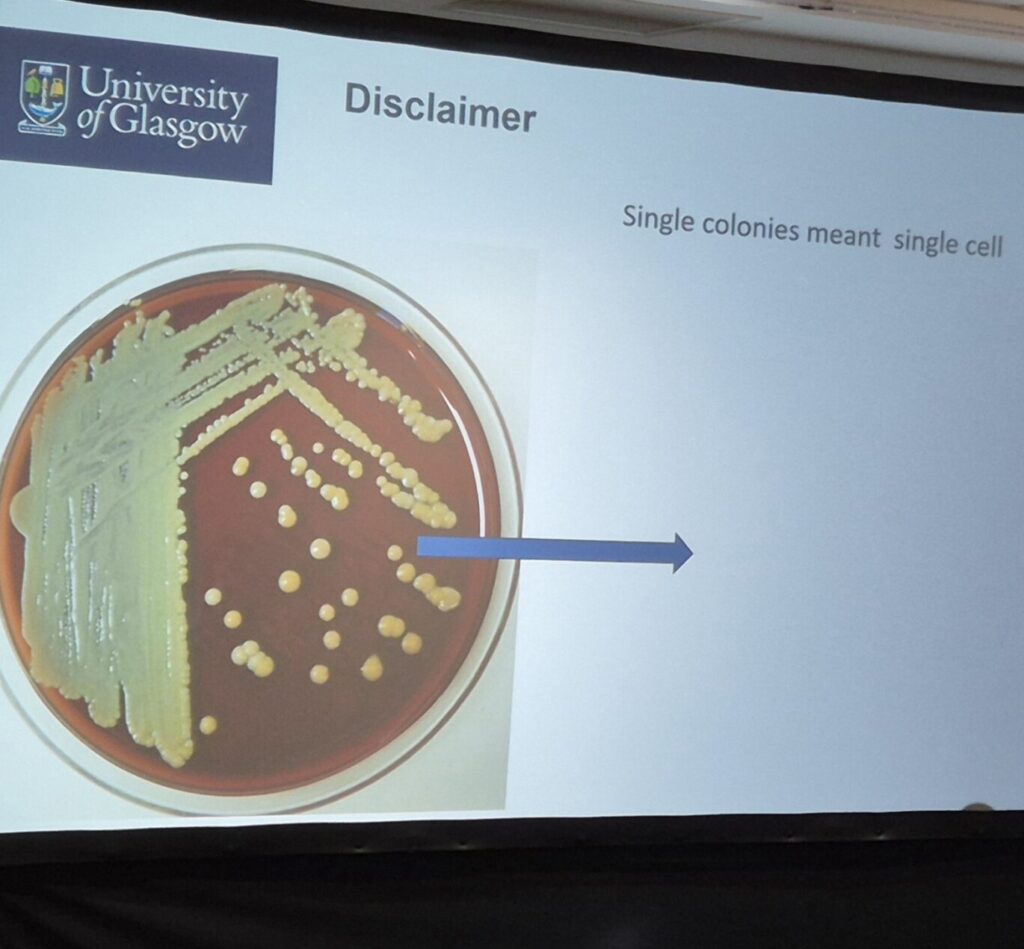
Professor Andrew Smith opened his session by challenging a common misconception: a single colony is far from a single cell. In fact, each visible colony contains millions of bacterial cells—so many that some experts consider a colony on an agar plate to be a simple form of biofilm.
A 12‑Hour Clock for 4 Billion Years

To set the scene, Andrew used a compelling evolutionary timeline:
- 12:00 – Earth’s crust solidifies (4 billion years ago)
- 2:05 – Archaea emerge, giving rise to today’s extremophiles
- 2:28 – Bacteria appear
- 10:40 – Early fish develop
- 11:21 – Mammals and dinosaurs
- 11:59 – Humans arrive—just two minutes before “midnight”
This striking timeline highlights bacteria’s immense evolutionary head start. Modern stromatolites—ancient, mushroom‑like structures formed by cyanobacteria—serve as ongoing reminders of this microbial legacy.
Biofilms in Unexpected Places

To illustrate bacterial resilience, Andrew shared findings from a Mexican cave system untouched by human activity. Researchers collected biofilm samples growing in thick mats on the cave walls. Remarkably, even without exposure to modern chemicals, some strains were naturally resistant to 14 antibiotics, demonstrating how bacteria are hard‑wired to survive extreme conditions
The Engineering Marvel of E. coli
A closer look at E. coli reveals billions of years of evolutionary refinement. Antibiotic‑resistant gram‑negative bacteria, for example, are encased in a dense polysaccharide capsule—raising the question: How do antimicrobial agents penetrate this barrier?
Add to that the rapid doubling rate of bacteria (1 → 2 → 4 → 8), and it becomes clear how quickly populations can explode.
Understanding Bacterial Growth
Andrew revisited the classic stages of bacterial growth:
- Lag Phase – Bacteria adapt to their environment.
- Log Phase – Exponential growth; the most reliable point for antimicrobial testing.
- Stationary Phase – Growth plateaus. Clinically, this is where phenomena like the Eagle effect emerge, where increasing penicillin doesn’t increase bacterial kill rate.
- Death Phase – Nutrients diminish and cells begin to die.
From MICs to EN Testing
Determining the Minimum Inhibitory Concentration (MIC) remains essential in understanding antimicrobial action. This principle translates into EN disinfectant testing, progressing from:
- Phase 1: Basic activity
- Phase 2 Step 1: Suspension tests
- Phase 2 Step 2: Practical carrier tests
- Phase 3: Optional in‑use/field trials
Biofilms: From Mushrooms to Cities
Traditional models depict biofilms as mushroom‑like structures attached to surfaces. New research, however, introduces the concept of a “liquid phase”, where free‑floating aggregates interact dynamically with their surroundings.
Biofilms are more like complex cities than solid masses—featuring channels, diverse architecture, and multiple microbial species collaborating (or competing). This complexity introduces additional challenges:
- VBNC cells – Alive but unculturable
- Persister cells – Temporarily stunned but capable of reactivating
- Dense extracellular matrices – Extremely difficult for detergents/disinfectants to penetrate
- Genetic exchange (“bacterial sex”) – Transformation, transduction, plasmid transfer, and even uptake of “naked DNA,” all contributing to heightened resistance
Build‑Up Biofilms: A Growing Concern
A 2019 study by MJ Alfa introduced the term “build-up biofilms”, highlighting how repeated cycles of use, hydration, disinfection, and storage create stubborn layers of dried organic matter and embedded microbes. The study calls for more stringent testing of cleaning equipment and manufacturer IFUs.
Currently, gaps remain in biofilm efficacy testing. Aside from ASTM and ISO 15883 cleaning models, harmonised European standards are still under discussion.

Andrew’s Call to Action
As the industry continues to explore improved testing methods, Andrew offered a practical roadmap:
- Get the basics right – Better IFUs, realistic challenges, proper validation, and periodic testing.
- Improve pre-cleaning compliance – Particularly with manual devices.
- Consider sterilisation for high‑risk scopes.

In the long term, Andrew suggests it may be time to move away from a “scorched earth” chemical-heavy approach. Emerging ideas include:
Micro robotics, highlighted in a recent state‑of‑the‑art review, which could one day reduce reliance on traditional endoscopes
Probiotic‑based strategies for medical devices
Hierarchy of controls to eliminate or substitute risks
Innovations like Colon Capsule Endoscopy (CCE) already in use in Scotland
Micro robotics, highlighted in a recent state‑of‑the‑art review, which could one day reduce reliance on traditional endoscopes
A Sound Barrier
Jim Tinsdeall delivered an insightful overview of sterile barrier systems used in the reprocessing of surgical instruments, focusing particularly on steam sterilisation. He began by highlighting the sector’s long-standing successes: for decades, surgical instruments have been safely reused following reprocessing, and confidence in sterility remains consistently high thanks to the solid foundations laid by previous generations.
Understanding the Basics
Jim revisited the fundamental principles of steam sterilisation, emphasising the essential steps for effective processing:
- Removing air from devices, packaging, or containers
- Ensuring full steam penetration to achieve adequate heating
- Allowing condensate to drain away
- Thoroughly drying the load to prevent microbial growth
- Maintaining the integrity of the barrier system until the point of use
- Avoiding contamination of the barrier itself
These principles underpin all types of sterile barrier systems currently in use.

Current Barrier System Options
Jim explored the main packaging solutions used across sterile services:
• Containers – A reusable, robust option with a high initial purchase cost but low ongoing cost per use. They require storage space, reprocessing, and can suffer damage such as bent lids. Many SSDs would like to transition fully to containers but are limited by wash capacity and available space. Aluminium containers, while durable and recyclable, typically have small filter areas and can be prone to knocks and dents.
• Single-use wrap – Consistent, reliable, and cost-effective, though vulnerable to tearing if mishandled. Traditionally made from cellulose, much of the market has now shifted to synthetic materials, raising concerns about sustainability and plastic reduction. Some products can be recycled, but many are incinerated.
• Fabric wraps – Reusable multiple times, offering low cost per use with modest initial investment. They require reprocessing, can be repaired, and are recyclable at end of life. Cotton has largely been replaced with synthetic fabrics in recent years.
• Peel pouches – An inexpensive, easy-to-use option that allows visual inspection of contents. Jim noted the mechanical stress these materials endure during sterilisation cycles.



Sustainability, Resources, and Future Thinking
Jim moved on to discuss the environmental landscape, noting the UK’s progress in renewable electricity generation, with 50% of supply coming from renewables over the past year. He highlighted ongoing challenges too, such as water collection and the environmental impact of plastics and polyfluoroalkyl substances (PFAS), often called “forever chemicals.”
He encouraged the sector to consider whether more products could become compostable, following trends seen in the food industry. Using Mentimeter, Jim invited the audience to share their priorities for an “ideal barrier system,” including whether compostable clinical waste might be feasible. He challenged delegates to imagine a future where bio‑digestion replaces incineration, contributing positively to renewable energy generation.



A Thoughtful Close

Jim concluded with a memorable proverb and a quote from the Dalai Lama XIV:
A fitting reminder that even small innovations can have a significant impact.
Keep a Lid On It? – Containerisation!
Dan Coole opened his session with a memorable anecdote about his very first encounter with rigid containers a decade ago. While in London on a Friday afternoon, he received an urgent call from a customer insisting, “I need some tins – I must get some tins!” Initially assuming they meant tins of beer, Dan soon learned they were referring to sterilisation containers urgently needed within a hospital. This moment marked the beginning of his journey into the world of container systems.

What Are Containers?
Dan explained that rigid containers—typically made from aluminium or stainless steel—provide a safe, validated method for sterilising, transporting and storing surgical instruments. Their dimensions are based on DIN standards, with heights up to 260 mm (most commonly around 200 mm). Width and length come in three primary sizes:
- Full size (1/1) – two filters
- Mid-size (3/1) – one filter
- Half size (2/1) – one filter
Size matters because transitioning from tray wraps to containers may require redistributing large instrument sets across multiple containers. This introduces challenges such as increased tracking complexity and weight limitations, which must align with manufacturer IFUs and sterilisation validation requirements.
Design, Materials & Features
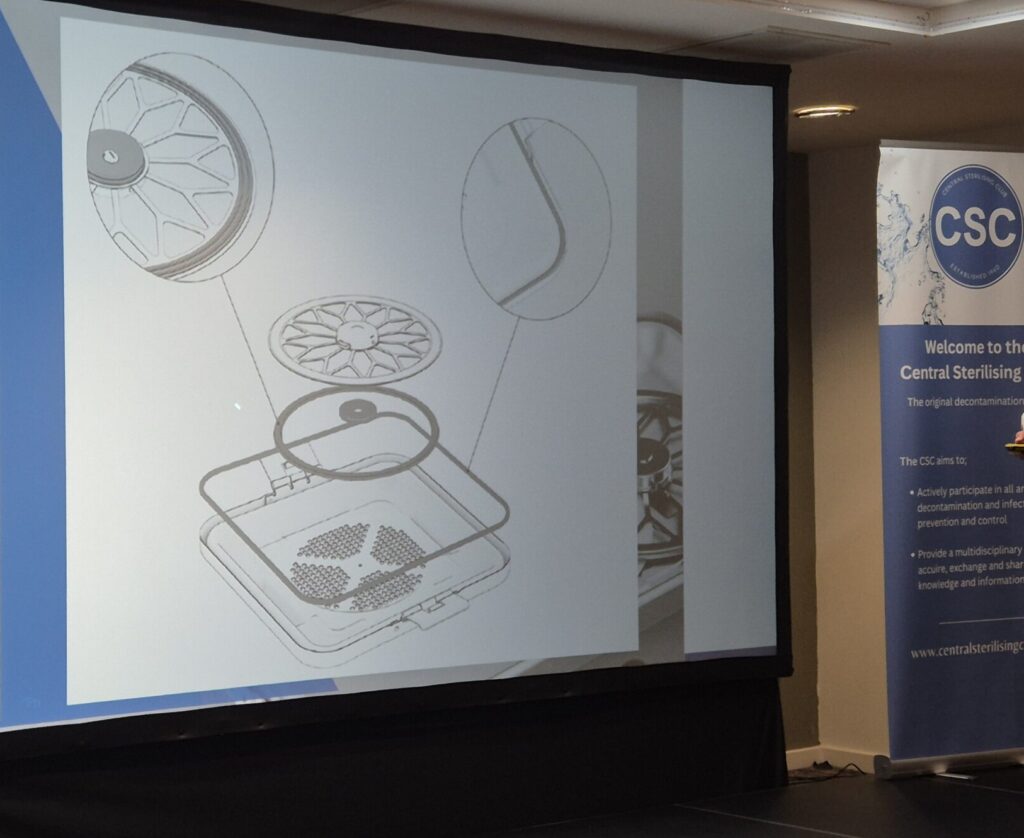
Containers typically include 1–2 microbial barrier filters in the lid. During sterilisation, steam penetrates the filter, sterilises the contents, and condenses during cooling. The effectiveness of this process relies heavily on:
- Intact gaskets around the lid and filter housing
- Appropriate seal materials (usually silicone, sometimes foam)
- Regular replacement or maintenance, depending on manufacturer guidance
Most systems use disposable filters, though reusable options are emerging as environmentally favourable alternatives.
Containers may also include:
- Coloured anodised lids for identification
- Tamper-evident locks
- Sterilisation indicators
- Traceability plaques
Materials are commonly either:
Stainless steel – highly durable and chemically resistant, but significantly heavier
Aluminium – lightweight, good heat conduction, easily coloured, but prone to denting
Manufacturing Standards & Testing
Containers are manufactured and validated against key standards including:
- ISO 11607 – packaging validation for sterility assurance
- HTM 01‑01 (and devolved equivalents)
- AAMI ST79 – biological testing guidance
Testing includes:
- Pressure/vacuum decay for air leak detection
- Sterilant penetration and microbial barrier integrity
- Dye penetration for gasket/filter seal testing
- Routine inspection of seals and mounts
- Drop tests and event‑related studies
- Accelerated and real‑time ageing studies
Notably, UK systems are typically validated for a 12‑month shelf life, whereas some European imports are validated for only 180 days, something purchasers must be mindful of.
Where Are Containers Made?
Germany is renowned for producing high‑quality validated container systems. Turkey also has a strong OEM manufacturing base supplying Europe, the US, and the UK. Lower‑cost systems tend to come from China and Pakistan. While the UK does not currently manufacture containers, domestic innovation has focused on RFID tracking and smart identification technologies.
Drivers for Change

Interest in container systems has increased largely due to the Department of Health’s “Design for Life” initiative, which promotes circular economy principles for medical devices. Containers support this model by being reusable, repairable, and ultimately recyclable.
Environmental considerations are a major driver:
A 2022 study by de Bruin showed containers may reduce CO₂ emissions by up to 85% compared to wrap. Additionally, many hospitals experience significant wrap damage. A UK study (2021–2022) found:
- 601 sets rejected due to wrap defects over 30 weeks
- Up to 13 same‑day case cancellations
- Most defects were holes or tears
Challenges in Real‑World Use
Dan emphasised that containers are not magic boxes. They introduce new challenges across the entire workflow:
- Preparation
- Sterilisation
- Post‑sterilisation handling
- Transport to theatre
- Use in theatre
- Return to decontamination
A comparison across two hospitals—one using wrap and one using containers—showed the container site required:
- Additional washers
- Extra space, power, water and chemistry
- Dedicated storage and racking
- Increased validation demands
The perceived need to switch to containers often stemmed from clinicians’ past experiences rather than user‑identified problems. Staff using wraps reported high confidence in wrap integrity thanks to easy visual inspection.
However, containers were recognised as excellent for off‑site use.
Evidence on Microbial Barrier Performance
Key research findings include:
- Shaffer (2015) – Wrap showed 0% contamination under challenge conditions; aged/damaged containers showed up to 87% contamination.
- Decarout et al. (2018) – Water leak tests may be effective in checking container seal integrity.
- Dunkelberg et al. (2006) – Wrap generally more consistent unless containers are rigorously maintained.
There are now emerging technologies for in‑situ integrity testing of containers.
Case Study: Cardiff & Vale Design for Life Pilot
The Trust evaluated using containers instead of tray wrap. Key findings:
- 60,000 wraps used yearly at a cost of £146k
- Projected annual saving: £61.5k
- CO₂ savings: >4,000 kg, equal to roughly six households’ annual consumption
Challenges included:
- Staff training
- Extra washer capacity required
- Complex traceability workflows
- High initial capital cost vs. managed service options
- Handling difficulties (weight, noise, ergonomics)
A phased introduction of 30–40% was recommended.
While containers cost approximately €2.00 per cycle, wraps ranged from €3.50–€4.00, suggesting quick payback—but many studies did not measure water or energy consumption, a significant oversight.
Maintenance Matters
To ensure container performance, consistent maintenance is essential:
- High‑pH detergents can damage anodised surfaces, creating a fine white residue
- Dents—especially on corners—affect lid seal contact
- Damaged gaskets can compromise sterility after processing
A preventative maintenance programme is crucial for reliability and sterility assurance.
Summary: When Containers Are Most Effective
Containers are ideal for:
- Large, complex surgical sets
- Heavy sets at risk of wrap tears
- High‑volume theatres and trauma centres
- Off‑site or mobile surgical units
- Field hospitals
- Environments where wrap damage is common
To Weave or Not to Weave – Is This Still a Question?

Linen may sit slightly outside the usual conversation around reusable medical device decontamination, but as Jincy Jerry reminded us, it remains a vital part of the wider decontamination landscape. Looking forward requires looking back—and Jincy opened her session by tracing the evolution of sterilisation itself.
A Look Back: From Carbolic Spray to Cutting‑Edge Technologies
The journey began with Joseph Lister, who introduced the carbolic spray machine into surgery, inspired by Louis Pasteur’s germ theory. His approach reduced infection rates from 50% to 15%—a remarkable leap forward.
From those early days, decontamination has evolved significantly:
- 1860s: Carbolic spray
- 1880s: Early autoclaves and steam sterilisation
- Mid‑20th century: Improved pressure and temperature controls
- 2000s: Plasma irradiation, vapourised hydrogen peroxide, and automation
This long arc of progress led Jincy to pose a provocative question: Have we “mutated” or truly “metamorphosed” as a field?
Mutation or Metamorphosis?
Jincy explored the difference.
- Mutation means incremental improvements—small changes to materials, design, and functionality.
- Metamorphosis is transformational—a fundamental redesign of philosophy and practice.
The move from woven textiles to non‑woven wraps, and eventually to rigid sterilisation containers, could be viewed as either—or both—depending on perspective.
These shifts, Jincy explained, have been driven by wider forces: growing healthcare demands, tighter regulations, rising sustainability expectations, and increasing automation.
Sustainability Pressures and the Challenge for Decontamination
The UK reprocesses millions of surgical instruments annually, yet no exact numbers exist. With Net Zero targets looming—originally requiring an 80% reduction by 2028, now shifted to 2032—the sustainability agenda is placing new scrutiny on decontamination.
Jincy highlighted several key concerns:
- Steam sterilisation demands significant energy and water
- Sterilisers remain idle nearly half the time, still consuming resources
- Packaging materials contribute notably to carbon footprint
Research shows that moving from woven to non‑woven wraps historically improved microbial protection and operational robustness. But with sustainability pressures mounting, some teams are questioning whether elements can be removed—and whether a return to linen might be feasible.
Jincy was clear: Sustainability matters, but never at the expense of patient safety.
The Reality of Linen Reprocessing
A 2022 study showed that incinerating single‑use packaging increases carbon footprint by 33–55%, whereas recycling could reduce it by up to 10%. This has prompted some hospitals to reconsider linen.
But Jincy urged caution.
She shared examples from laundry facilities across England and Ireland—raising serious concerns about compliance, cleanliness, and process safety. Key issues included:
- Overuse of red “infected” bags
- Manual opening of bags, contrary to HTM 01‑04 guidance
- Excessive dust and fluff in “dirty” and even “clean” zones
- Linen dragged on floors during drying and processing
- Wet, hot linen packed too quickly
- Performance targets that incentivise speed over safety
All of this, she noted, creates risks—including documented outbreaks of Bacillus cereus linked to laundered linen.
Instrument Sterilisation: Hidden Microbial Risks
Even within high‑temperature sterilisation processes, contamination risks persist. Jincy referenced a UK investigation where 15 orthopaedic patients developed endophthalmitis. Staph. aureus and Bacillus species were found inside packaging and on instruments due to poor autoclave maintenance and handling failures.
Further studies show that while instruments inside rigid containers remain sterile, the outer surfaces—and the hospital environments they pass through—carry significant microbial loads.
The Carbon Cost of Linen Loss
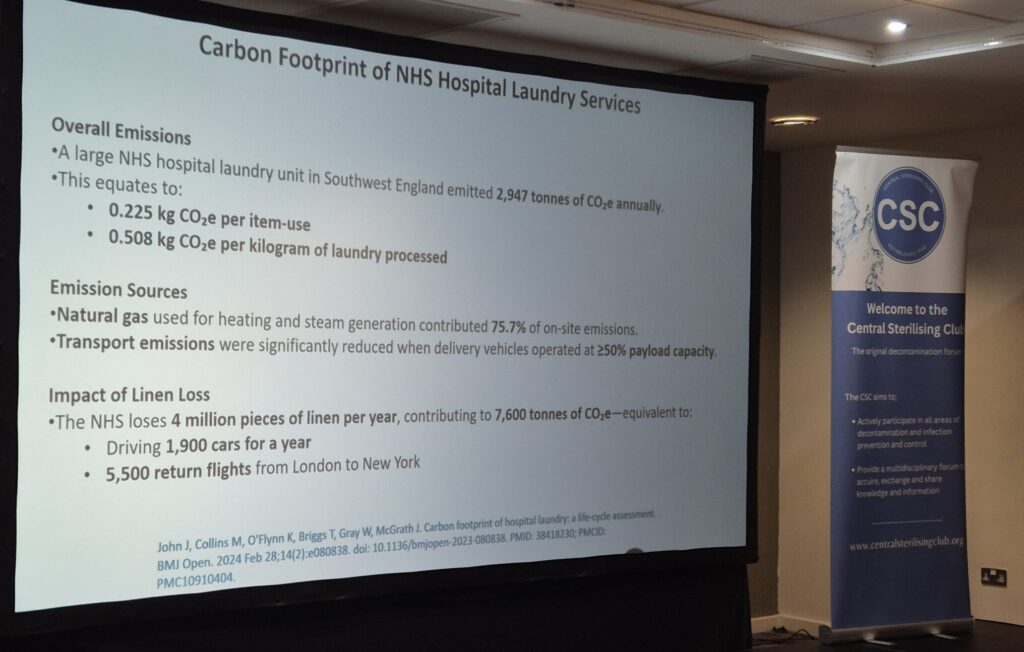
A 2024 study found the NHS loses 4 million pieces of linen every year, contributing an estimated 7,600 tonnes of CO₂e—equivalent to:
- 1,900 cars driven for a year, or
- 5,500 return flights from London to New York
With figures like this, the sustainability case for linen becomes even more complex.
A Final Question
After reviewing the risks, inefficiencies, and environmental impact, Jincy left the audience with a powerful closing thought:

Audience participation with Q&A
Click on the image to access the free recording of this session

Rethink, Revise, Rebuild; Co-Creating for a Better HTM Panel Discussion
Click on the image to access the free recording of this session

A Right FANdango – A Merry Dance with Fans!
In this lively and eye‑opening session, Gail Lusardi explored a deceptively simple question: what really happens when we switch on a fan in a healthcare environment?
Although not traditionally linked to the decontamination of reusable medical devices, fans can be found everywhere—from sterile services to endoscopy units—and their impact on infection prevention and control (IPC) is far from trivial.

Fans: Comfort vs. Consequence
Portable fans have long been a go‑to when warmer weather arrives, and with 2025 officially declared the UK’s hottest summer on record, their use is only increasing. As temperatures and humidity rise due to climate change, so too does the risk of infection—raising important questions for IPC teams.
Gail and her colleagues set out to answer two key questions:
• What are the risks associated with using portable fans?
• How can those risks be mitigated in the absence of strong guidance?
A Variety of Fans… With One Common Problem
Healthcare environments use a surprising range of fan types:
- Bladed
- Bladeless
- Handheld
- Desktop
- Floor‑standing
- Ceiling‑mounted
However, none of these are designed specifically for healthcare use. This means no clear instructions for safe cleaning, decontamination, maintenance, or repair—despite variations in size, noise, airflow, and power usage that all influence risk.
The Hidden Costs of Keeping Cool
Running a single fan for 24 hours costs around £0.23/hour. Multiply that across 5 fans in 10 areas and the figure quickly climbs to £1,000 per month.
This pales, however, beside the financial impact of healthcare-associated infections: a single Clostridium difficile case can cost £7,000–£10,000, with Wales reporting quarterly C. diff costs between £1.7M and £2.4M in 2023–24.
How Fans Really Work—and Why That Matters
Fans don’t cool rooms; they simply move air, creating a wind‑chill effect. In fact, the motor generates additional heat, feeding it back into the environment.
Bladeless fans, although marketed as safer, still rely on hidden blades in the base that draw in and push out air.
In clinical settings filled with microorganisms—some able to survive hours to years outside the body—any device that moves air also redistributes these particles. The COVID‑19 pandemic heightened awareness of how aerosols travel, reinforcing concerns around airborne spread.
The Microbiome, Dust, and Environmental Contamination
Every person carries a unique microbiome, shedding skin cells daily—making up to 40% of household dust. In healthcare settings, this shedding contributes to environmental microbial load. Coupled with high bed occupancy, reduced cleaning opportunities, and rising antimicrobial resistance, the risk of healthcare‑associated infection increases.
Different areas of skin harbour different organisms, highlighting the importance of appropriate decontamination, especially during procedures involving skin contact.

Limited Guidance Leaves Many Questions
Currently, guidance is sparse—mainly the NHS Wales Estates Alert (EFA) 2019 on portable fans and the Scottish and Welsh Infection Control Cleaning Standards. This gap leaves IPC teams navigating complex risks with limited direction.
Fans and the Hierarchy of Controls
Gail explored where fans sit within the hierarchy of controls:
- Elimination: Not realistic without risking heat stress or discomfort.
- Engineering controls: Ideally all facilities would meet HTM ventilation standards, but ageing estates make this challenging.
- Alternative solutions: Options such as heat‑repellent window films, external blinds, or canopies—already common in hotter countries—may offer future solutions for the UK.
- Substitution: Cooling strategies (e.g., showers) aren’t always feasible, especially for immobile patients.
If Fans Must Be Used: Placement Matters
A thorough risk assessment is essential. Gail recommends:
- Positioning fans to blow towards an open window, not directly at people.
- Keeping them at bed/chair height or higher.
- Ensuring airflow does not sweep across surfaces or out through doorways.
- Never using fans during sterile or aseptic procedures.
Final Thoughts
Fans may be simple devices, but their use in healthcare is anything but straightforward. Effective management must address not just the type of fan, but also location, cleaning, maintenance, storage, and reuse.
Gail concluded with a clear call for innovation: it’s time for fans designed specifically for healthcare settings—built with IPC at their core.
Physical Vapour Deposition: Why Surface Quality Matters

Physicist and nanotechnology specialist Alistair Kean shared a fascinating look into the world of Physical Vapour Deposition (PVD)—a cutting‑edge coating technique used across industries, including healthcare. His talk highlighted not only how PVD works but also why the condition of a product’s surface is crucial to achieving high‑performance coatings.
What Is PVD?
PVD is a physics‑based vacuum‑coating process where a target material is vaporised using heat, electrons, or plasma. The resulting atoms then condense onto a product’s surface, forming an exceptionally hard and adherent coating. This makes PVD ideal for high‑demand environments—such as oil and gas drilling—and adaptable for many other applications, from food packaging and jewellery to electronics and surgical instruments.
Because the technique is scalable, PVD can transition easily from research laboratories to full industrial production.
Key Advantages of PVD Coatings
- Superior adhesion
- High resistance to wear, corrosion, and tear
- Enhanced hardness
- Controlled, uniform thickness, typically around 1 micron
- Versatility, compatible with many substrates
- Environmentally friendly, producing minimal waste
Limitations and Material Considerations
PVD is a line‑of‑sight technique, meaning the coating is deposited onto surfaces directly facing the vapour source. While rotating 3D objects helps, complex internal structures—like lumens in endoscopes—are better suited to chemical coating methods.
Material quality matters too. For instance, 316L stainless steel, the highest‑grade variant, offers strong corrosion resistance. When paired with PVD coatings, it performs reliably even in harsh environments such as saline (sea water) testing, which is known for its aggressive corrosive properties.
Real‑World Applications
One example Alistair shared was the coating of bionic hand electrodes—where one side is coated with a titanium alloy and the other with ultra‑pure gold to achieve optimal performance.
Why Surface Preparation Is Critical
Before any coating is applied, surface quality must be meticulously controlled. This includes understanding:
- Surface roughness and topology
- Chemical composition and existing bonds
- Any prior treatments
To achieve the required cleanliness, products undergo glow discharge plasma cleaning. In this process, argon gas ions bombard the surface, stripping away contaminants and leaving behind free atomic bonds. This atomically clean surface allows the incoming coating atoms to chemically bond with high strength—one of the reasons PVD coatings are so robust.
Nature‑Inspired Antimicrobial Research
With over 20 years of research into antimicrobial coatings—including work with copper, silver, and nanoparticles—Alistair is now exploring innovations inspired by nature. One remarkable example: insect wings. Their surfaces, covered in nano‑sized pillars, naturally resist contamination and remain self‑disinfecting. Mimicking these structures is opening new pathways for future antimicrobial technologies.
A Thoughtful Quote to close by Alexander von Humboldt (1769–1859)
“Our imagination is struck by what is great: but the lover of natural philosophy should reflect equally on little things.”

Thank YOU
As we conclude this report, we extend our sincere thanks to all our speakers, delegates, the organising committee, and the AV support team for helping make the Autumn Study Day 2025 such a successful and enjoyable event.
If you attended as a delegate and would like access to the event recordings, please contact the CSC Media and Editor Officer at [email protected].
For those who were unable to attend but would like to listen to selected talks, these are available through the provided link for a small fee, which supports our not‑for‑profit club and the events we deliver.



